Redefining Emergency Medicine Excellence Through
Continuous Process Improvement
Our goal at Emergency Care Partners (ECP) is to improve patient experience and satisfaction by optimizing emergency department throughput, highlighting areas of opportunities that yield the biggest improvements, and assist in change management and implementation.
Electronic Medical Record (EMR) Data Integration
to Drive Process Improvement
We integrate with a hospital’s EMR to enable our regional emergency medicine groups better manage patient volume, optimize coverage, and evaluate provider productivity which ultimately optimizes emergency department throughput.
Standard inbuilt reports providing valuable insights which can be used to evaluate baseline processes in the emergency department and identify target areas for improvement by automatically compiling reports from different sources.
Daily/weekly/monthly automatic reports sent directly from the ECP Analytics platform to facilitate continuous monitoring and control.
Customizable data visualizations with ability to be drilled down to the specific patient level. Project-specific reports built on demand to rapidly assist in pilot improvement projects and initiatives.
Continuous data validation helping to provide governance around clinical quality measures by identifying inconsistent and missing data.
Automatic alerts on critical measures to notify process owners of any deviations from Key Performance Indicator (KPI) goals.
Discrete Event Simulation Modeling and Analysis.
Billing Reconciliation
Patient Census Tracking
Accurate Reporting
ED Flow Simulator
Emergency Care Partner’s Senior Industrial Engineer, walks through and demonstrates a discrete event simulation model. The simulation was created leveraging the integrated EMR data from a partner group’s hospital.
Doing More with Data
Dr. Mark Laperouse, Chief Medical Officer at Professional Emergency Physician Associates (PEPA) talks about how they are leveraging data to customize solutions and improve outcomes in the emergency departments they serve.
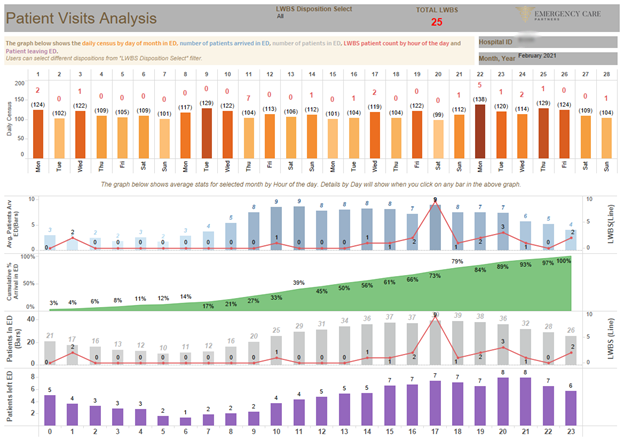
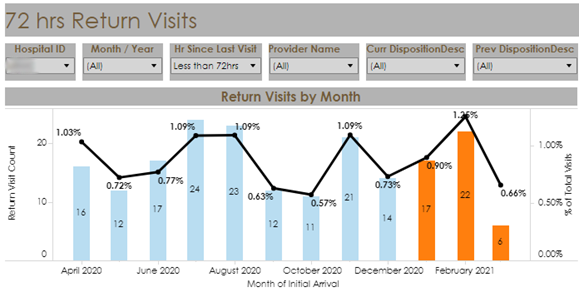
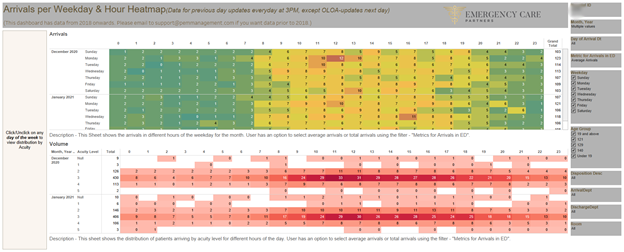
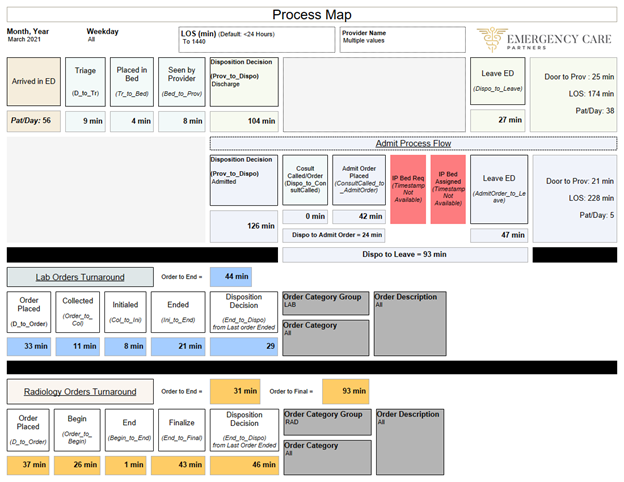
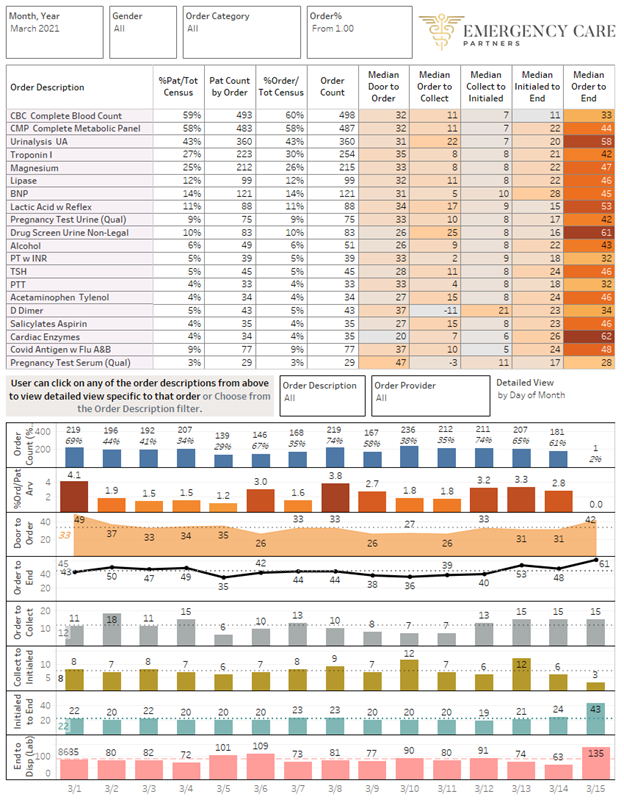
Examples Snapshots from Emergency Care Partners Analytics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}